Thomas Gant is a PhD student funded by the NIHR Biomedical Research Centre: Maudsley at the Institute of Psychiatry, Psychology & Neuroscience. Amy Grant is a lived experience researcher employed by South London and Maudsley NHS Foundation Trust working on the SloMo2 implementation-effectiveness study.
In this blog they discuss how lived experience expertise has helped redesign a digital therapy for paranoia – SloMo – to support translation into real world services. This process has recently been written up as a paper in the journal JMIR Human Factors.
Worries about harm from others (sometimes termed paranoia) involve beliefs that other people intend to harm, threaten, or act against you. These experiences are one of the most common difficulties in psychosis and can make everyday interactions feel threatening or unsafe.
Cognitive behavioural therapy for psychosis is recommended for people experiencing paranoia. However, delivering psychological therapies in ways that are accessible, engaging and inclusive remains an ongoing challenge.
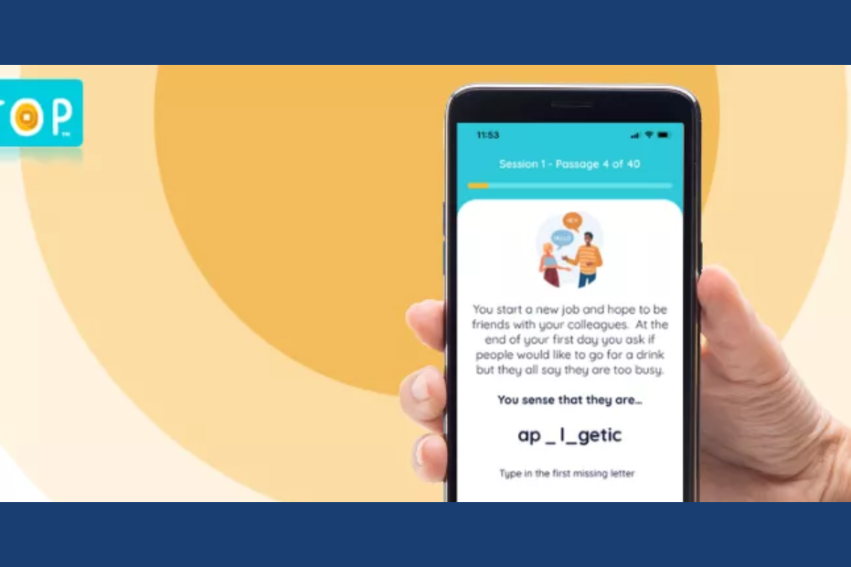
To address these limitations, our colleagues at King’s College London developed a digitally supported therapy targeting worries about harm from others, SloMo. It includes an online platform used during sessions with a therapist, alongside a mobile app that helps service users practise skills in their daily lives.
In a randomised controlled trial, SloMo showed promising outcomes. But as our team began thinking about the next stage of the project, an important question emerged: how could we optimise the technology so it could move beyond research and into routine care?
Bridging the evidence-to-practice gap
Many digital therapies never make the transition from research into real-world services, despite encouraging findings – a problem often described as the evidence-to-practice gap.
One reason is that digital therapies are not always designed with the experiences of people who use them in mind. If a system feels clunky, irrelevant, or disconnected from people’s experiences, it is unlikely to be adopted in busy and financially stretched services.
As part of the SloMo redesign work, we set out to optimise the software so that the therapy felt usable, engaging and inclusive within routine NHS care.
Designing with end users in mind
To do this, we used a co-design approach, working closely with the people who would ultimately use the technology: service users and therapists.
We brought together a transdisciplinary team including lived experience researchers and consultants, clinicians, software developers and designers.
We began by reviewing findings from the original SloMo trial and speaking with people who had previously taken part in the therapy to better understand their experiences. These insights highlighted several areas where the platform could be improved with the broad aim of improving user experience and inclusivity.
Turning feedback into design changes
In workshops, we translated these insights into design improvements. Often this involved looking beyond what users initially said they wanted in order to understand underlying needs.
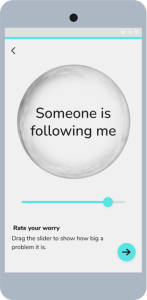
SloMo encourages people to represent their worries in digital “worry bubbles”, which they can resize during therapy to reflect changes in how distressing those worries feel. Early idea testing suggested that participants preferred pinch interactions for resizing worry bubbles within the app, as this felt more engaging and interactive. However, after testing prototypes that included both pinch and slider gestures, participants ultimately favoured the slider option because it was simpler and more intuitive to use, particularly for those with lower confidence in using technology.
Learning from lived experience
One of the most valuable aspects of the redesign process was the sustained involvement of people with lived experience. This took several forms, including co-design workshops, consultation with independent lived experience experts and oversight from a Lived Experience Advisory Panel.
One discussion that stood out to both of us during the redesign process was around the language used within a newly developed module which focused on altered perceptual experiences. The module was initially titled “unusual experiences”, a phrase commonly used in CBT for psychosis but through the discussion it became clear that the phrase ‘unusual experience’ sounded like it was coming from an outside perspective of someone trying to describe what someone is going through. Instead it was suggested that renaming the module to ‘when the world doesn’t feel right’ would sound more like a personal, first-hand experience. Indeed, lived experience experts describe psychosis and paranoia as ‘the world feels wrong’, ‘everything feels different’ and ‘the world feels confusing and not real.’
Looking ahead
The redesigned software is now being tested in an implementation study across three NHS Trusts. This study will evaluate both how the therapy is used in routine care and its effectiveness for paranoia, wellbeing, and goal attainment.
If digital therapies are to move beyond research studies and into routine practice, they need to be designed with real-world care in mind from the start. Bringing together clinical, research and lived experience perspectives helped shape a version of SloMo designed for the realities of routine care.
Watch a short film on how lived experience has shaped SloMo
This film was made as part of Wellcome’s Health Wonders series, marking its 90th anniversary in 2026.
Links
- Gant T, Taylor KM, Ward T, Garety P, Hardy A; Optimizing SloMo, a Digitally Supported Therapy Targeting Paranoia, for Implementation: Inclusive, Human-Centered Design Study, JMIR Hum Factors 2025;12:e75377, doi: 10.2196/75377
- Visit the SloMo website
- Thomas Gant, NIHR BRC: Maudsley PhD Student