

Jessica Wilkins is a psychologist and PhD candidate with the Centre for Research in Eating and Weight Disorders (CREW) at the IoPPN. This study is part of the EDIFY programme, which brings together researchers from different disciplines to understand why young people develop eating disorders, how these illnesses progress, and how recovery can be better supported.
Eating disorders are serious mental illnesses that affect psychological and physical health, and social functioning. Although effective treatments are available, many people with eating disorders find it difficult to seek help. People from minoritised groups experience eating disorders at similar rates to the wider population but are less likely to access treatment. Because help-seeking research has largely relied on clinical samples, the experiences of people who do not access treatment may be missed. This is particularly important for under-served groups, who are often under-represented in both treatment settings and research.
Whose experiences are missing in eating disorders research?
To identify groups that may be under-served in eating disorder research and treatment, we conducted focus groups with people with lived experience and clinicians. These discussions, alongside a review of the existing literature, informed our decision to focus on men, people from sexual and gender minority groups, and people from minoritised ethnic backgrounds. We worked closely with organisations supporting these individuals and adapted our research procedures to facilitate participation, including providing remuneration and offering different ways to take part, such as written responses.
Exploring help-seeking through an intersectional lens
We conducted 17 interviews with people with lived experience of an eating disorder who self-identified as belonging to an under-served group in eating disorder research. Importantly, participants were not required to have a formal eating disorder diagnosis or treatment history to take part.
As part of the interviews, we adapted Duckworth and Hankivsky’s Wheel of Power and Privilege for a UK context and for the experiences of people with eating disorders. We renamed it the “Wheel of Social Locations” and used it to facilitate discussions with participants about how different social characteristics may shape experiences of power, marginalisation, and discrimination. Most participants identified more than one, often intersecting, social characteristic that influenced their experiences of seeking help for an eating disorder using this wheel.
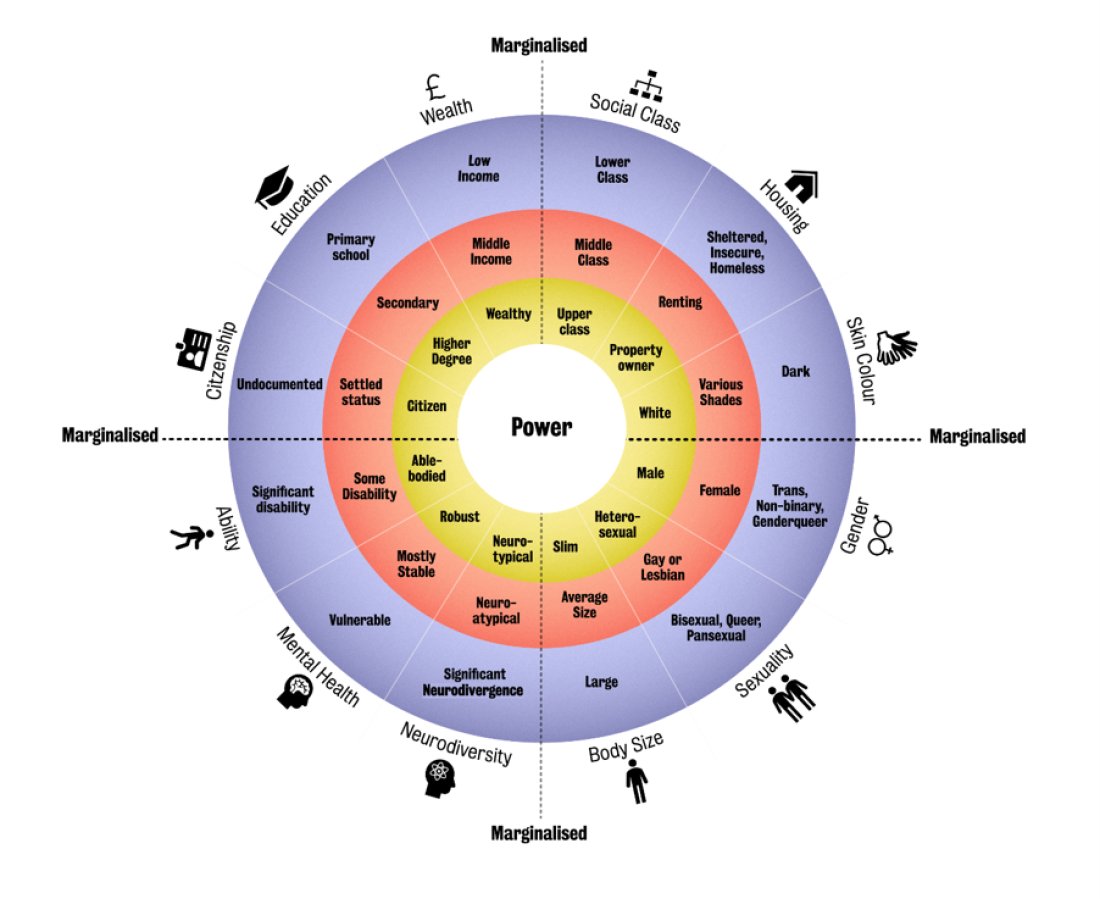
CREW Wheel of Social Locations Adapted from Duckworth and Hankivsky’s Wheel of Power/Privilege, this figure includes additional marginalised characteristics relevant to the experiences of individuals with eating disorders in the UK. Proximity to the centre represents greater social power and privilege, while increasing distance from the centre reflects greater risk of marginalisation.
Key findings
Our findings confirmed and extended existing evidence on help-seeking for eating disorders. Participants described a range of barriers and facilitators, which we organised across individual, interpersonal and community, and structural or systemic levels.
One of the most important individual-level barriers was internalised shame. Many participants were aware of common stereotypes about the “type” of person who develops an eating disorder. Because they did not see themselves reflected in these stereotypes, they often questioned the legitimacy of their symptoms. For some, this made it difficult to recognise the severity of their illness; for others, it reinforced beliefs that they did not deserve care.
I didn’t know much about binge eating, so I didn’t know I could ask for help for that. I thought that was just me being, you know, greedy…asking for help when I look the way I do just felt really, really embarrassing and like they were going to laugh or judge me or just dismiss me. – Participant Quote, a woman of mixed ethnic background with binge eating disorder
These stereotypes also shaped participants’ interactions with others, including family members, friends, and healthcare professionals. Our analysis highlighted how barriers to help-seeking can be layered and intersecting. For example, men from minoritised ethnic backgrounds described navigating both gendered and culturally mediated beliefs that discouraged discussing mental health difficulties, creating additional barriers to seeking support.
I have had negative experiences with the GP, though in regard to like my weight and stuff…they would immediately just assume it was a weight loss issue as opposed to…a mental health issue. – Participant Quote, a man of mixed ethnic background with binge eatng disorder
Participants also identified several systemic barriers to accessing care. These included difficulties obtaining treatment when living with co-occurring physical or mental health conditions, as well as restrictive service eligibility criteria, such as BMI thresholds and limited service provision for certain eating disorder diagnoses.
I don’t really relate to a lot of the ways that eating disorders are defined and described and that kind of stuff. I don’t know, I feel quite excluded from a lot of them in terms of even the symptoms. -Participant Quote, a man with anorexia nervosa and ARFID
Alongside these barriers, participants identified several factors that facilitated help-seeking. Access to online information and resources supported help-seeking by increasing understanding of eating disorders and providing greater visibility of people with similar social characteristics, for example, shared ethnic and gender backgrounds.
Turning Findings into Better Care
Based on our findings, we developed several clinical and policy recommendations to improve help-seeking for eating disorders by people from under-served groups:
- Developing targeted awareness-raising and psychoeducation programmes that address internalised shame, reduce stigma, and challenge common stereotypes about eating disorders. Findings from this study informed the development of a series of awareness-raising animations, available on the EDIFY website (see below).
- Improve the accessibility of eating disorder services by ensuring facilities can accommodate individuals with diverse body sizes and accessibility needs, including appropriate scales and furniture, and lifts that can be accessed independently.
- Address systemic barriers to help-seeking by removing BMI thresholds for access to treatment and ensuring services are commissioned for all eating disorder diagnoses, in line with NICE guidelines.
This research was supported by the National Institute for Health and Care Research (NIHR) Biomedical Research Centre (BRC): Maudsley.


